Nutcracker Syndrome

Nutcracker Syndrome (NCS), aka left renal vein compression syndrome, arises when the left renal vein (LRV) is compressed, leading to a range of symptoms. The most common symptoms include left flank pain, hematuria/proteinuria, and pelvic pain. This compression typically occurs due to the anatomical positioning of the Superior Mesenteric Artery (SMA) and the abdominal aorta, which function like a "nutcracker" limiting outflow of venous blood in the LRV. This results in abnormally elevated venous blood pressure within the LRV, which in turn causes the associated symptoms.
Importantly, compression of the LRV can also be observed on CT scans or other imaging modalities in approximately 25% of the general population without any accompanying symptoms. This asymptomatic condition is referred to as Nutcracker Phenomenon (NCP), distinguishing it from Nutcracker Syndrome, which is characterized by the presence of clinical symptoms. As such, NCP is not considered pathological, as varying degrees of LRV compression are commonly found in many individuals without causing any health issues.
ANATOMIC CONFIGURATIONS
There are several anatomic configuration to the Nutcracker anatomy due to variance in embryogenic processes. We will consider three main ones that affects NCS.
1. Anterior Configuration: most commonly occurring, the left renal vein (LRV) passes between the narrowed space of SMA and the aorta
2. Posterior or retroaortic Configuration: next most commonly occurring, the LRV passes behind the aorta where LRV is compressed between the aorta and spine.
3. Circumaoritc Configuration: in more rare circumstances, there’s two LRV; one passing anteriorly, and another one passing posteriorly to the aorta; you can consider this as combined anterior and posterior LRV existing together.
In anterior configuration, the SMA and aorta are nearly parallel, and this is called narrow aortomesenteric angle, causing “nutcracker” phenomenon that “squeezes” the LRV in between aorta and SMA. In posterior NCS configuration, it is the aorta and the spine that causes the compression. In circumaortic NCS configuration, it is both the SMA and spine with aorta in between that can cause the compression. All the configurations described can be found in general population without symptoms.


Posterior
Anterior


Aortomesenteric Angle
Circumaortic
VARIANT ANATOMIES
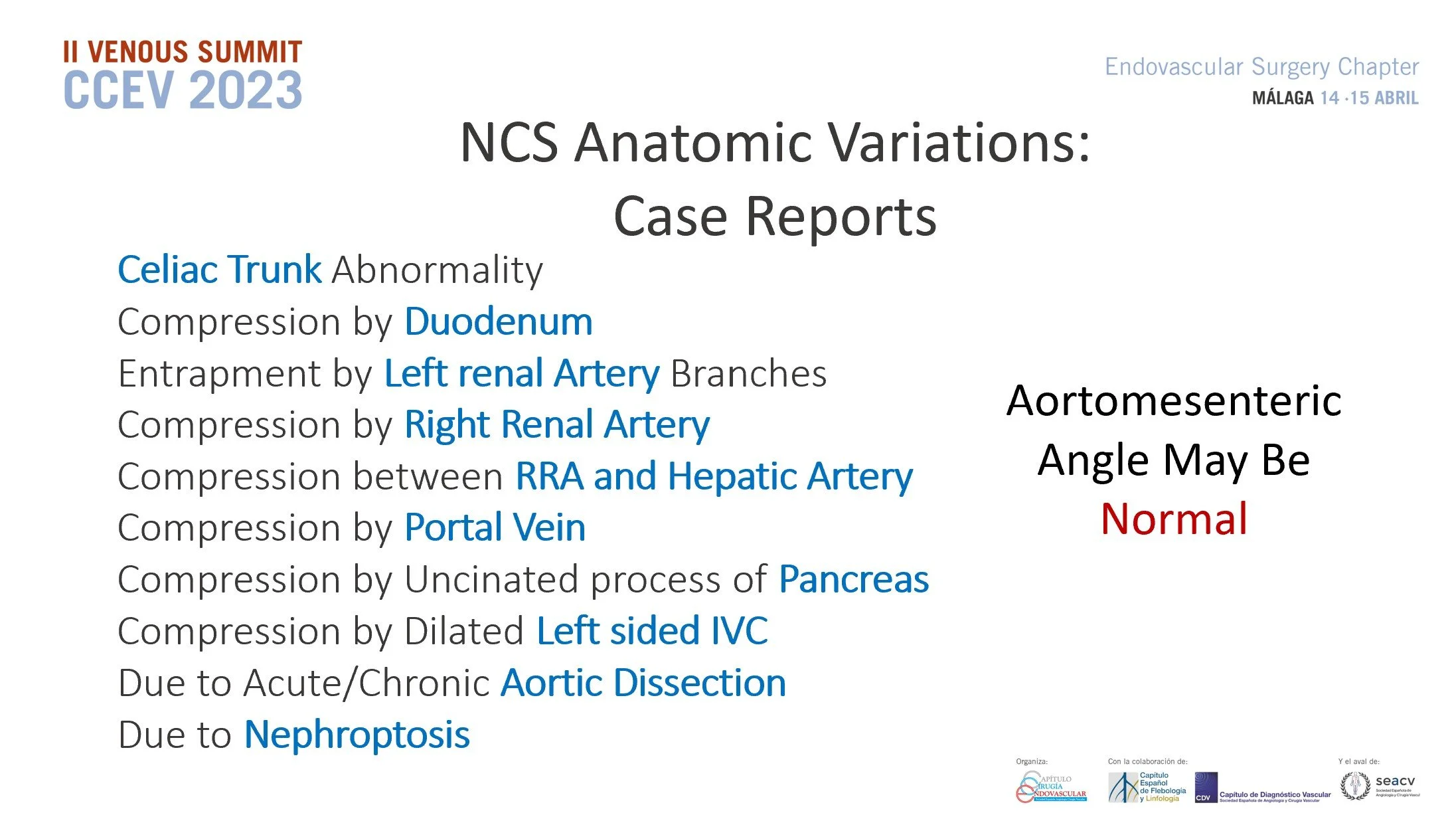
It’s not always the superior mesenteric artery that causes the left renal vein compression. More rarely, it can be the right renal artery, a portion of the small bowel called the duodenum, or head of the pancreas that can also cause the LRV compression, and in these cases the aortomesenteric angle can be normal. Sometimes it’s the high arching spine condition called lordosis that displaces the aorta anteriorly, causing the left renal vein to be tented or stretched causing the compression. Another rare type is nephroptosis when the kidneys are mobile, and standing up can cause it to descend enough to create a kink causing the compressive effect. A mass effect of tumor or other abnormal structures also can externally compress it as well.
So, just because the CT/MR/US doesn’t show the narrow aortomesenteric angle, it doesn’t always mean NCS is ruled out. These variant NCS anatomy can be often missed on routine radiology reports.

Duodenum Compressing LRV

Right Renal Artery Compressing LRV
Copyright Kurtis Kim 2023
SYMPTOMS
Symptoms of NCS is quite vast, not just what the textbooks describe here:
Left flank pain
Blood in the Urine
Pelvic Pain
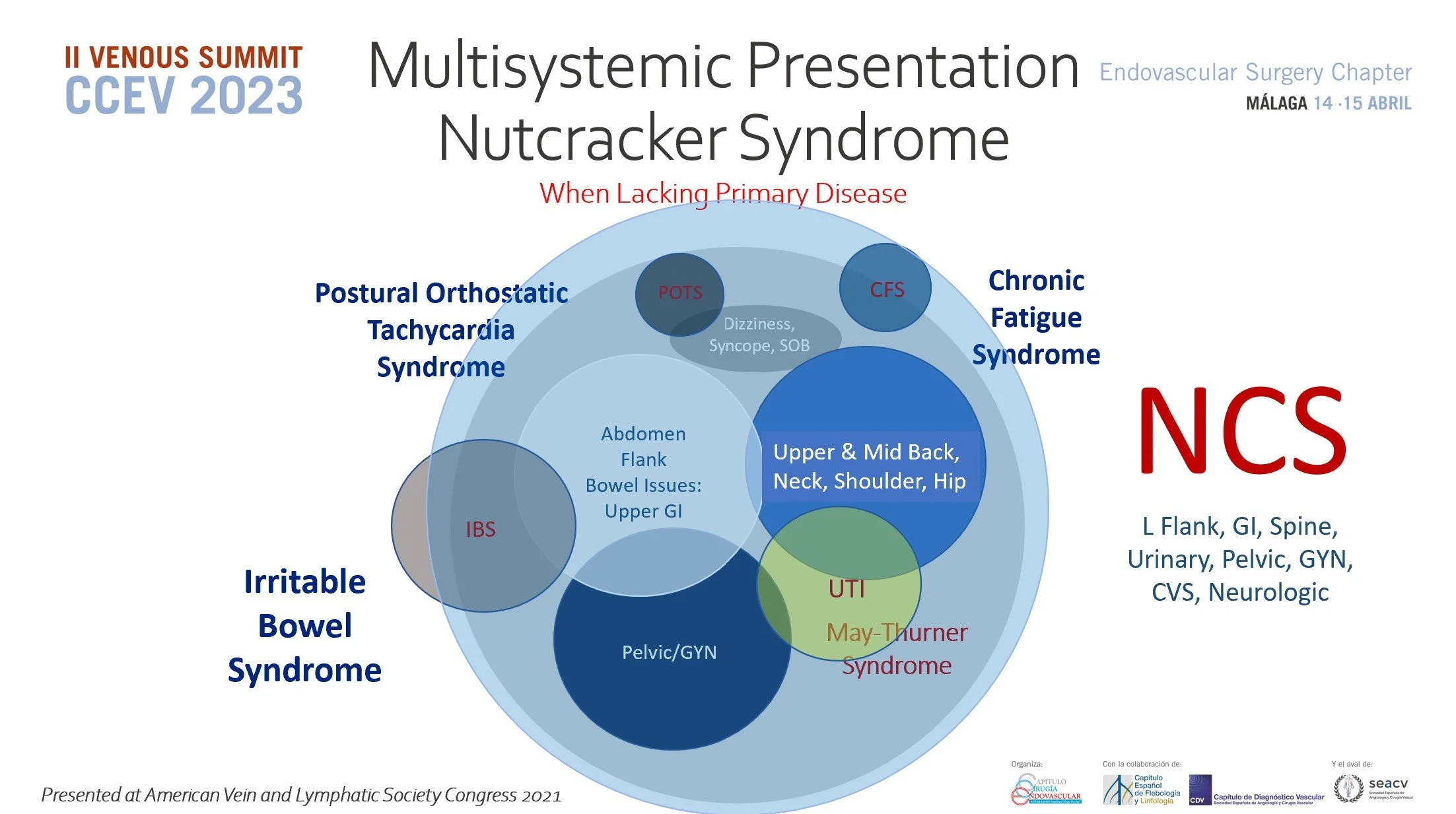
We understand patients symptoms do not always align perfectly with all three diagnostic criteria. There has been growing awareness, newly proposed guidelines, and emerging case reports that delve into both typical and atypical symptom presentations. To better classify these, we categorize t them as "primary" and "secondary" symptoms for clarity.
Primary Symptoms are the triads described above. These are the symptoms we expect to resolve after surgery. However there are also a proposed guideline that makes hematuria not a necessary component of the diagnosis.
Secondary Symptoms are ones that are not a part of the triad, but has been shown to improve on subset of patients. While there are more common causes of these symptoms, NCS has a clear role in many of them shown below. This diagram has been presented at several leading vascular symposiums in USA, Europe, and Asia.
Headache Migraines
DIAGNOSTIC WORKUP
Ultrasound | CT | MR
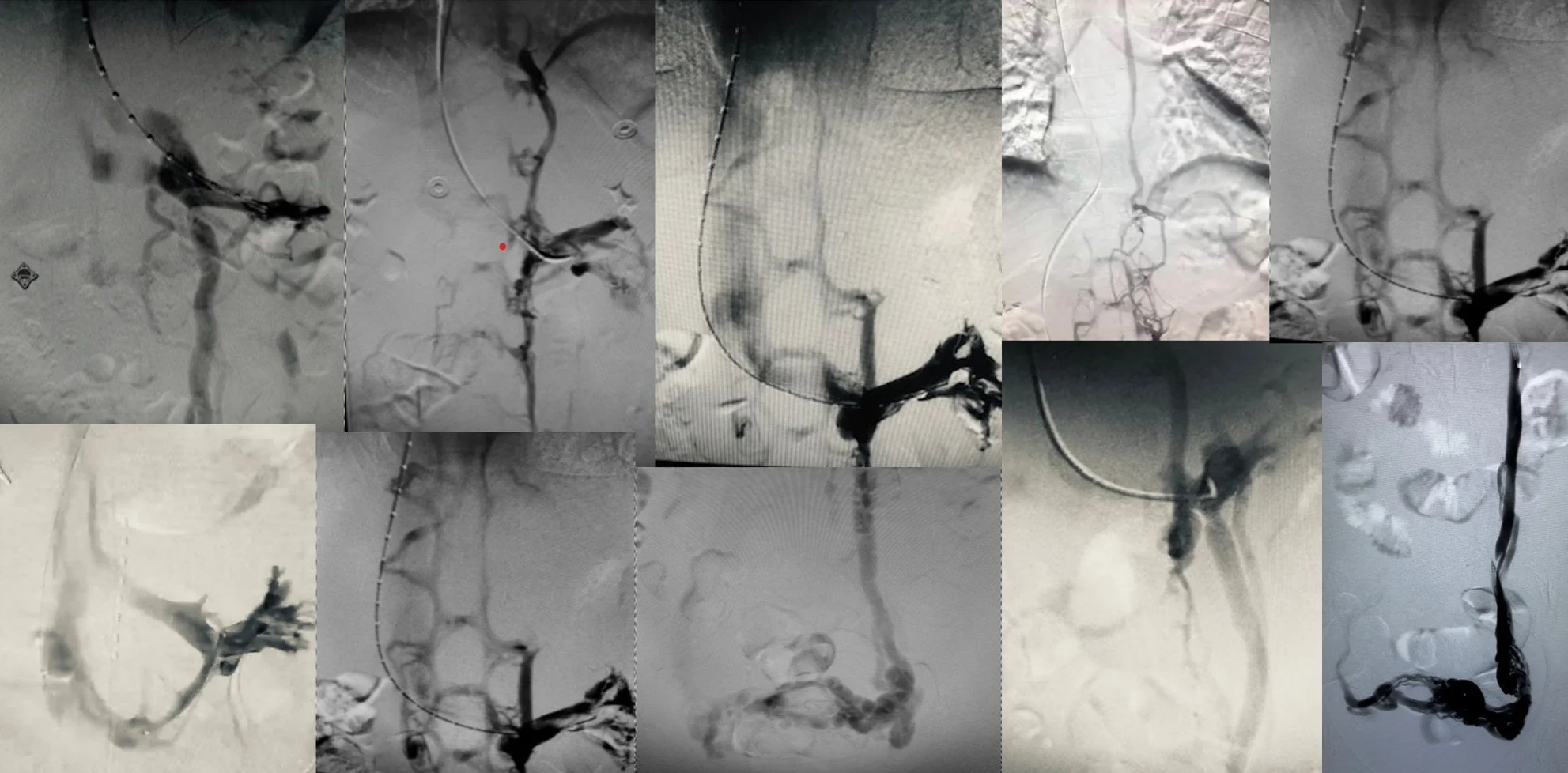
Venogram with Intravascular Ultrasound (IVUS) is the Gold Standard Test for NCS
Many faces of Nutcracker Syndrome Venograms Each Presenting with Different Sets of Symptoms
TREATMENT OPTIONS
The management of NCS involves a spectrum of surgical interventions, each tailored to address the unique needs of individual patients. Factors such as the patient’s specific presenting symptoms, anatomical variations, history of prior surgeries, and personal preferences play a critical role in determining the most appropriate approach. It is important to note that no single surgical procedure is universally optimal or suitable for all cases. Surgical options include:
Endovascular Stenting of Left Renal Vein
Extravascular Stenting of Left Renal Vein
Left Renal Vein Transposition
Reno-Caval or Reno-Splenal Bypass
Autotransplantation of Left Kidney
Left Ovarian Vein Transposition
Nephropexy, (Donor)Nephrectomy